|
When we have persistent pain, want to get stronger, want to make a change to our lifestyle, improve our body image, etc. We generally start by looking for the quick solution. As a culture we have become use to scouring the internet looking for a quick fix. We think that there must be some type of pill we can take or machine we can buy. We are so used to instant gratification that we believe everything should be this way. Well I got news for you when trying to make true long-term changes to pain or your overall health there is no quick fix that can replace putting in the hard work and consistency with things like diet, exercise, and sleep.
I have many patients that ask me about different products that they see in infomercials about rubbing on this cream for back pain, using a certain pillow to fix their neck, or getting this machine that they can put there feet on while they are sitting that will help them with their neck pain. My response to these patients is always the same. We can not expect a passive solution to fix your active problem. We need to seek active solutions for our active issues. If I have persistent low-back pain that is preventing me from being able to perform my normal exercise regimen of weight-training and running I should not expect that using some pain relieving gel will magically make it better. Now I am not trying to say that some of these passive solutions do not have any merit or use at all but we need to see them for what they are and use them as such. Things that I mentioned earlier such as pain relieving topical creams, pills, an expensive vibrating massage chair, insert about a thousand other late night infomercial products here. These are all things that can provide some symptom relief but they are not going to be the solution to your problem. I would even take this one step further and add things like getting a massage, injections, dry needling, and even some surgical procedures to this list. If you are working with someone and they are using these techniques as the sole solution to your issue then it is time for you to find someone else to help you. As I stated earlier I am not saying that some of these things shouldn't be used I believe that there is great value in being able to alter a person’s symptoms, but that should be just the beginning. To go back to the idea of having back pain that prevents a person from performing a weight training regimen, we could perform some type of massage or give them a cortisone injection to help with their pain and they would be feeling pretty good. Now what do you think that person is going to do? They are going to go back to the gym throw on the same weight that they had been trying to do and are going to perform their squats in the same way that they always have, and likely going to experience the same pain that they always have. Now it may not be right away, but that pain will be back. However, if we can take this same person and we actually look at their movement patterns and assess whether or not they have the mobility and motor control to perform the squat correctly, now we can make a true change and allow the person to have the kind of long-term outcome that they are looking for. Taking this more active approach of improving movement patterns does not come easy, but without it most people will not see the kind of change that they want. So it is time to understand that the vast majority of the time we are not going to be able to find some quick fix or passive solution to our problems or toward reaching our health/fitness goals. We need to learn to move correctly, build true strength, and be consistent with good lifestyle choices. So, the solution is simple, it is whether or not we are in the correct mindset and are willing to build the habits that is most often the true barriers to our success. Now quit scouring the internet for the easy way out, because most likely there is not one anyway, and get moving toward reaching your Prime!
0 Comments
We are not always going to be able to train completely pain-free, and having pain in our low-back while trying to perform different variations of the squat is one of the more common complaints that you will hear from people that engage in strength training. Most often our intuition would tell us that if I am having pain in my back than my problem must be in my back. So people will resort to performing some sort of stretching and core strengthening routine to make their back more mobile and strong. This can be part of the answer, but for many this will not lead to the effect on their symptoms that they were hoping for. For these people often times the cause of their pain is something wrong with the squat movement pattern itself, and the key to fixing this issue is often all the way down at the ankle. When a person does not have the necessary ankle mobility to get into a full squat position it can lead to compensation in which we may utilize increased amounts of lumbar and hip flexion to get all the way to the bottom of the squat. This can lead to increased shear forces in the lumbar spine, especially as the load/weight increases. In these cases it can help to be able to perform the squat with a more upright torso. However, to get into a more upright torso position a person will need to have the prerequisite ankle mobility to do so. When talking ankle mobility most people just think about ankle dorsiflexion as it relates to proper squat mechanics, however it can be just as important to have proper tibial internal rotation and lateral tibial glide. In this week’s blog we will discuss the concepts of ankle dorsiflexion, tibial internal rotation, and lateral tibial glide. We will talk about how each impacts the squat pattern and give an example of a simple mobilization to address decreased mobility in these ankle movements. Ankle Dorsiflexion Ankle dorsiflexion refers to the ability to bend the foot backwards bringing your toes closer to your shin, this would be in a non-weight bearing position just moving your foot. However, when we are in a weight-bearing position the foot will be fixed and so it is more about how well can the tibia slide anteriorly over the dome of the talus, essentially meaning can the knee go in front of the toes while being able to keep the foot flat on the ground. When performing a full squat with decreased ankle dorsiflexion a person will increase the forward angle of their torso to allow for full squat which can then lead to increased load and shear forces of the lumbar spine. Ankle dorsiflexion can be assessed by the ankle lunge test, which is performed with a person standing or in a half-kneeling position and they move their knee forward in an attempt to touch it to the wall and is scored by the distance that the big toe is from the wall. A normal amount of dorsiflexion is considered 4 inches from the wall. 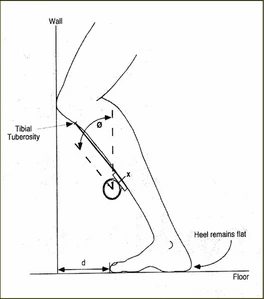 To improve ankle dorsiflexion you can simply perform the ankle lunge test by trying to touch your knee to the wall and keeping the foot flat. To increase the mobilization I prefer using banded distraction to apply a posterior force to the dome of the talus. As seen in the picture below, utilize a band around the front of your ankle joint with the band placed below the two large bones on both sides of the ankle called the medial and lateral malleoli. Then just like the ankle lunge test or stretch attempt to lunge forward pushing the knee over the toes of the foot keeping the foot flat on the ground. Perform the mobilization for 1-2 minutes.  Tibial Internal Rotation Internal rotation of the tibia helps to keep the knee in line with the foot during a full squat. Having good tibial internal rotation and help to allow for a more forward foot position in the squat will help to minimize medial knee collapse during the squat leading to a more stable position of the squat. The more efficient the pattern the better we are able to use the hip and knee musculature to manage the load being lifted reducing the stress to the lumbar spine and associated musculature. It is tested in the seated position with a person placing weight through their heel and then attempt to point the toes toward the inside as far as possible, a normal test is when the knee is in line with the third toe.  To perform mobilizations for tibial internal rotation you can use the same banded technique as for ankle dorsiflexion, but point the toes as far inward as possible with keeping the knee straight and then perform your lunge again for 1-2 minutes. An alternative if you do not have access to a band is pictured below. Place foot on a stool, box, step etc. then place hands around you lower leg and apply a rotary force toward the inside sustain that force as you lunge forward and back. Again to keep it simple perform for 1-2 minutes.  Lateral Tibial Glide Lateral tibial glide describes the ability of the tibia to glide over the dome of the talus to the outside of the ankle. This allows for an improved ability to maintain the knees in a wider position in the squat which allows for a more upright torso angle as a person is able to bring their hips more straight down between their feet instead of having to lean forward at the trunk and torso to get into the full squat position. This will reduce lumbar flexion shear forces produced during the movement, and also, as described with tibial internal rotation, it will lead to better efficiency in using the hip and knee musculature to perform the movement which also reduces load to the lumbar spine and associated musculature. Pictured below is a common assessment for looking at lateral glide of the tibia. You can see here that the foot is being maintained in a flat position on the ground and the knee is being allowed to drop to outside as far as it can before the inside of the foot comes off the ground. The normal range is considered to be a 30 degree angle from the foot the knee.  To perform a mobilization to improve lateral tibial glide get into the lunge position and use the opposite hand to brace the foot into position and then use hand on same side to give help give downward and outward pressure to the leg as you perform a lunge motion. This can be seen in the picture below. Can also perform with foot on top of a box. Again we suggest 1-2 minutes.  These are all great mobilizations that will help to improve ankle mobility. However, if you only perform them in isolation you will not get the effects that you are really looking for. As with all mobilizations the new movement gained from the mobilization works best if it is able to be put immediately into practice. These should be programmed in on days in which your workout will be involving some sort of squat pattern work. When really tight it can work well to perform these mobilization between sets. We always need to understand that when dealing with the human body the work is never done, so if you find that mobilizing your ankles improves your squat pattern and any pain associated with it, this is something that should be incorporated into your normal movement practice. It takes consistency to make something become a habit and to become a Prime Mover!
It is commonplace in our current healthcare system for people to hear, “If insert common activity or movement here is bothering you than just stop doing that” or “You know that you should not be doing that.” The problem with this is that sometimes the things we are being told to avoid are things that are essential to our everyday life or are an integral part of the activity that we want to perform. Here are two recent examples that I have seen in my own practice of such a thing happening. The first was an elderly patient that hurt his back while gardening because he was attempting to lift a bag of soil out of his truck. He was told by his physician that he knows better than to be lifting things. This is a man that still lives at home, how is it possible for him to continue with his normal way of life and avoid all lifting. The second example of suggesting activity avoidance as a treatment option was a 16 yo female athlete being treated for persistent knee pain linked to patellofemoral issues, and whom had underwent arthroscopic meniscal debridement approx 3 months prior, sidenote the surgery had no effect on her knee pain. This patient was told by her surgeon that she should go to physical therapy but not perform any squatting exercises since that hurts, but that she could return to basketball. In this situation we are expecting someone that cannot tolerate squatting to be able to work their way back into a sport that requires cutting and jumping, which are activities that lead to much greater compression and shearing forces at the knee. Which from a training perspective, how are we going to be able to return someone to basketball without being able to train the squat pattern, a very fundamental piece of jumping and landing.
In both of the above situations the suggestions of avoiding the given activities were impractical for the situations. If we have discovered weaknesses in a person's fundamental movement patterns, such as the hinge in the elderly man, or the squat in the female athlete, should these not be things we are looking to improve instead of avoid. I would agree with the physicians that both of these patients were in a position in which their physical capacity did not match up with the physical demands being placed on their bodies during the activities each person wanted to do. However, I do not agree that the answer is to avoid these activities, as common sense would tell us that if we avoid an activity how will our body ever develop to capacity to perform it. Instead of avoiding these activities we need to train them, and that is exactly what we did in both scenarios. In both cases we began with looking at the person’s movement patterns to look for either mobility deficits that would not allow them to perform the movements fully, or motor control issues that cause them to have poor techniques despite having the necessary joint range of motion and soft-tissue flexibility. Once you are able to determine the limiting factor, which could be both, the solution to the problem becomes simple. Prescribe the necessary mobility and motor control exercises to improve movement quality. Then scale the movements in a way that allows the patient to perform the movement successfully and progressively load the pattern. Often times we like to make musculoskeletal issues more complex than they have to be. There is nothing tricky about the two cases described here and so the solution does not need to be tricky either. A weakness in both patients was identified and a progressive loading strategy for the patterns in which they were weak were created to improve their physical capacity to perform the desired tasks. The only tricky part is getting the person to understand how consistent and diligent we must be if we want to make true changes to our movement patterns and improve our physical capacity. To recap, please stop telling people that they can not do things or that they must avoid certain activities because they are causing a pain stimulus. Instead let's teach people how to move correctly and show them how to progressively strengthen themselves, as this is were a true resiliency against injury occurs. |
Archives
January 2020
Categories |
 RSS Feed
RSS Feed
